Otitis Media Infection Treatment: Effective Relief & Prevention
Effective Treatments for Otitis Media Infections
Few things are as disruptive as the sudden, sharp pain of an earache. Whether you are an adult experiencing a sudden reduction in your hearing accompanied by deep pressure, or a parent trying to soothe a crying child in the middle of the night, dealing with a middle ear infection can be an exhausting ordeal. Scientifically known as otitis media, this condition is one of the most common reasons for medical visits worldwide.
Finding an effective otitis-media-infection-treatment is critical not only for immediate comfort but also for preventing long-term damage to the delicate structures of the ear. While many ear infections resolve on their own, understanding the nuances of the condition—from identifying symptoms and managing pain to knowing when medical intervention is necessary—empowers you to make the best health decisions.
In this comprehensive guide, we will explore everything you need to know about navigating a middle ear infection. We will dive deep into causes, diagnostics, home remedies, medical treatments, and surgical options, ensuring you have a complete roadmap to ear health.
Understanding Otitis Media: The Anatomy of a Middle Ear Infection
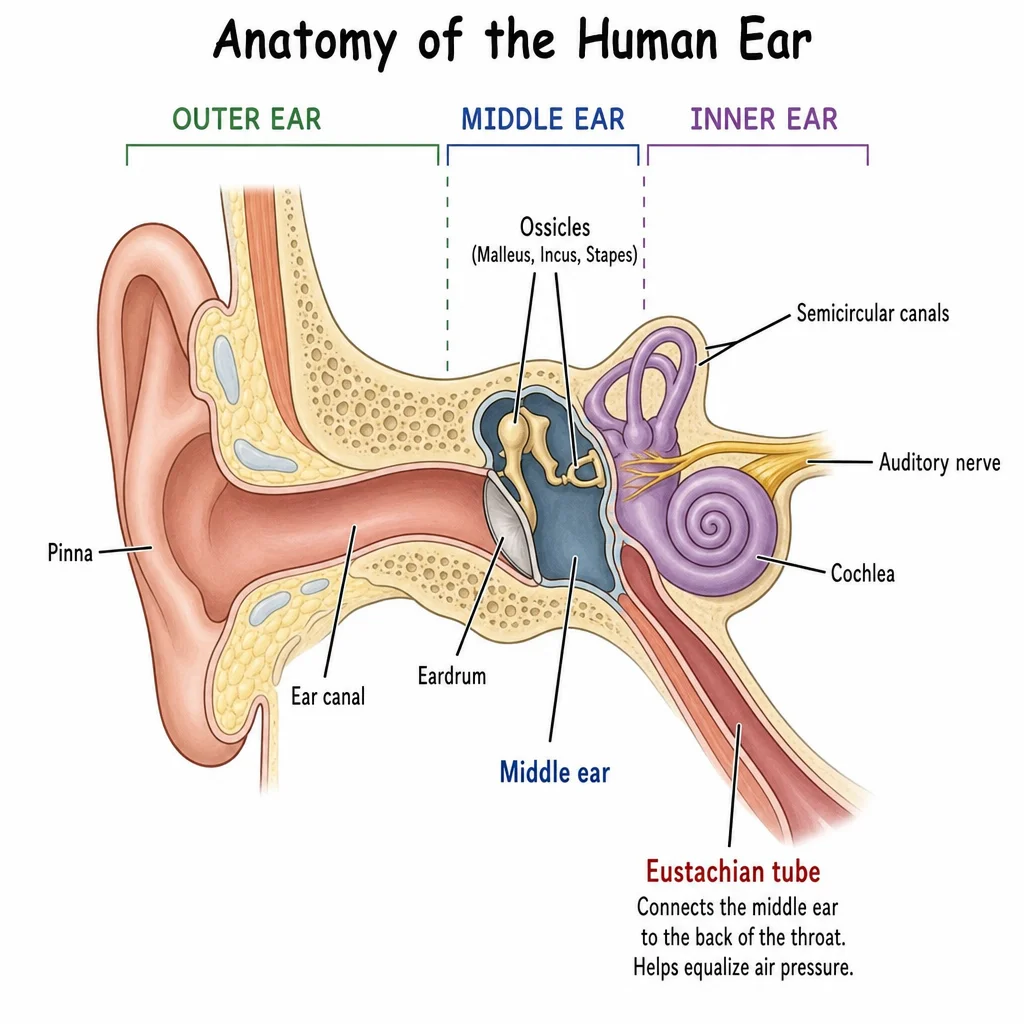
To truly understand how to treat an ear infection, it helps to know exactly where and how it occurs. The human ear is divided into three parts: the outer ear, the middle ear, and the inner ear.
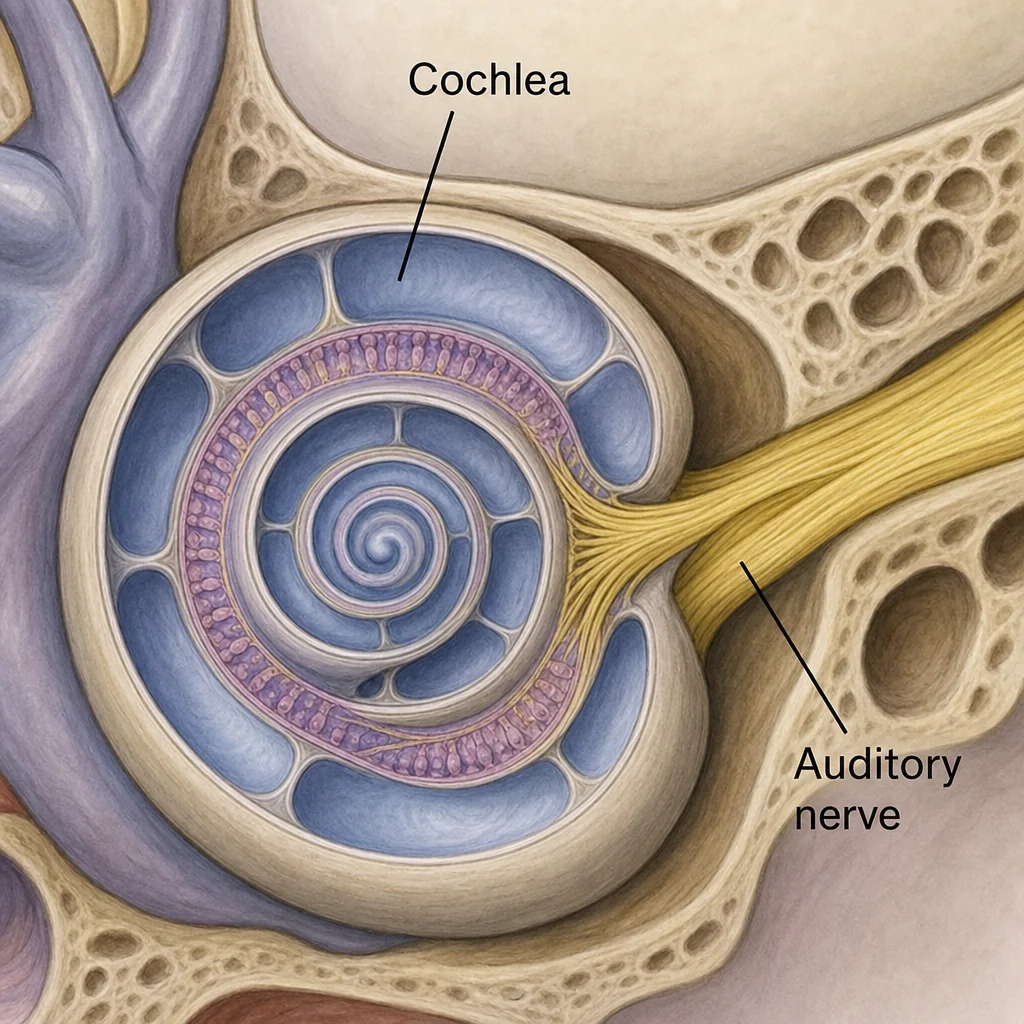
Otitis media specifically targets the middle ear—the small, air-filled space located just behind the eardrum (tympanic membrane). This space contains three tiny bones (the ossicles) that transmit sound vibrations from the eardrum to the inner ear.
The middle ear is connected to the back of the throat by a narrow channel called the Eustachian tube. This tube has a vital job: it regulates air pressure inside the middle ear, refreshes the air, and drains normal secretions. However, when the Eustachian tube becomes swollen or blocked—often due to a cold, flu, allergies, or respiratory infection—fluid becomes trapped in the middle ear. This dark, warm, and moist environment is the perfect breeding ground for bacteria and viruses.
The Three Main Types of Otitis Media
Not all middle ear issues are identical. Medical professionals generally categorize otitis media into three distinct types, each requiring a different approach to care:
Acute Otitis Media (AOM): This is the classic "ear infection." It involves a sudden onset of infection in the middle ear. The trapped fluid becomes infected, leading to inflammation, bulging of the eardrum, redness, and acute pain. Often, it is accompanied by a fever.
Otitis Media with Effusion (OME): Sometimes, after an active infection has cleared up, fluid remains trapped behind the eardrum. OME can also occur without a prior infection due to non-infectious Eustachian tube blockages. It usually doesn’t cause sharp pain, but it can create a feeling of fullness and muffle your hearing.
Chronic Suppurative Otitis Media (CSOM): If an ear infection persists for a long time or keeps returning, it is considered chronic. CSOM can lead to ongoing damage to the middle ear and the eardrum, often resulting in persistent ear drainage and more severe hearing issues.
Recognizing the Signs and Symptoms
The symptoms of an ear infection can vary wildly depending on the patient's age and the severity of the infection. Because children are disproportionately affected by this condition, identifying the signs early is a crucial part of the otitis-media-infection-treatment process.
Symptoms in Adults and Older Children
For adults and older children who can vocalize their discomfort, the symptoms are usually straightforward:
Deep, throbbing pain inside the ear
A feeling of pressure or fullness in the ear
Muffled hearing or a ringing sensation (tinnitus)
Fluid draining from the ear (if the eardrum has ruptured)
Dizziness or a loss of balance
A low-grade fever
Acute Otitis Media Symptoms in Toddlers and Infants
Babies and toddlers cannot easily communicate where they hurt, making diagnosis trickier for parents. Recognizing acute otitis media symptoms in toddlers requires careful observation. Look for these behavioral and physical cues:
Tugging or pulling at the ears: While babies sometimes pull their ears out of habit or teething pain, doing so alongside other symptoms is a strong indicator of an ear issue.
Increased crying and fussiness: Especially when lying down, as horizontal positions increase pressure on the middle ear.
Changes in sleeping and eating habits: The pain of chewing or sucking can make feeding agonizing, leading to a loss of appetite.
Unexplained fever: Often ranging from 100°F to 104°F.
Clumsiness or balance issues: The ear plays a massive role in equilibrium; fluid buildup can cause a toddler to become unusually unsteady on their feet.
Fluid drainage: Yellow, brown, or white fluid seeping from the ear canal.
Distinguishing the Cause: Bacterial vs Viral Ear Infection Signs
One of the most complex aspects of treating otitis media is determining its root cause. Infections can be triggered by either viruses or bacteria, and this distinction dictates the course of treatment.
Understanding bacterial vs viral ear infection signs can help set expectations for recovery.
Viral Ear Infections: These almost always accompany or immediately follow an upper respiratory infection (like the common cold). The symptoms build up gradually. If the patient has a runny nose, a cough, and a sore throat along with ear pain, a virus is often the culprit. Viral infections do not respond to antibiotics and typically clear up on their own as the immune system fights off the primary virus.
Bacterial Ear Infections: These can also follow a cold, but they tend to strike with sudden, severe intensity. The pain is usually localized to one ear, and the patient may spike a higher fever. If symptoms persist for more than three to four days without improvement, or if they rapidly worsen, bacteria like Streptococcus pneumoniae or Haemophilus influenzae are likely responsible.
The Diagnostic Process
If you suspect you or your child has an ear infection, a visit to a healthcare provider is the safest route. Doctors use several tools to get a clear picture of what is happening behind the eardrum.
The Otoscopic Examination
The cornerstone of diagnosing middle ear issues is the otoscope, a lighted instrument used to peer inside the ear canal. A healthy eardrum looks pearly gray and translucent. During an active Acute Otitis Media (AOM) infection, the doctor will likely see an eardrum that is red, swollen, and bulging outward due to the pressure of the infected pus behind it.
Pneumatic Otoscopy
To check for fluid, a doctor might use a pneumatic otoscope. This device gently puffs a small amount of air against the eardrum. A normal eardrum will move back and forth easily in response to the air pressure. If the middle ear is filled with fluid, the eardrum will be rigid and show little to no movement.
Otitis Media with Effusion Diagnosis
An otitis media with effusion diagnosis can sometimes be tricky because the patient usually does not have an active fever or severe pain. The doctor will look for air bubbles or a visible fluid level behind the eardrum. In cases where the fluid has been present for a long time, they may recommend tympanometry. This test uses a small device placed in the ear canal to measure the acoustic reflex and air pressure of the middle ear, providing a highly accurate graph of how much fluid is trapped and how well the eardrum is functioning.

Immediate Relief: Pain Management Strategies
Regardless of whether an infection is viral or bacterial, the priority for the patient is almost always the same: stopping the pain. The pressure from trapped fluid stretching the sensitive eardrum can be excruciating. Effective earache treatment focuses on reducing inflammation and easing discomfort while the body (or medication) fights the infection.
How to Relieve Middle Ear Pain in Adults
When figuring out how to relieve middle ear pain, adults have several accessible options:
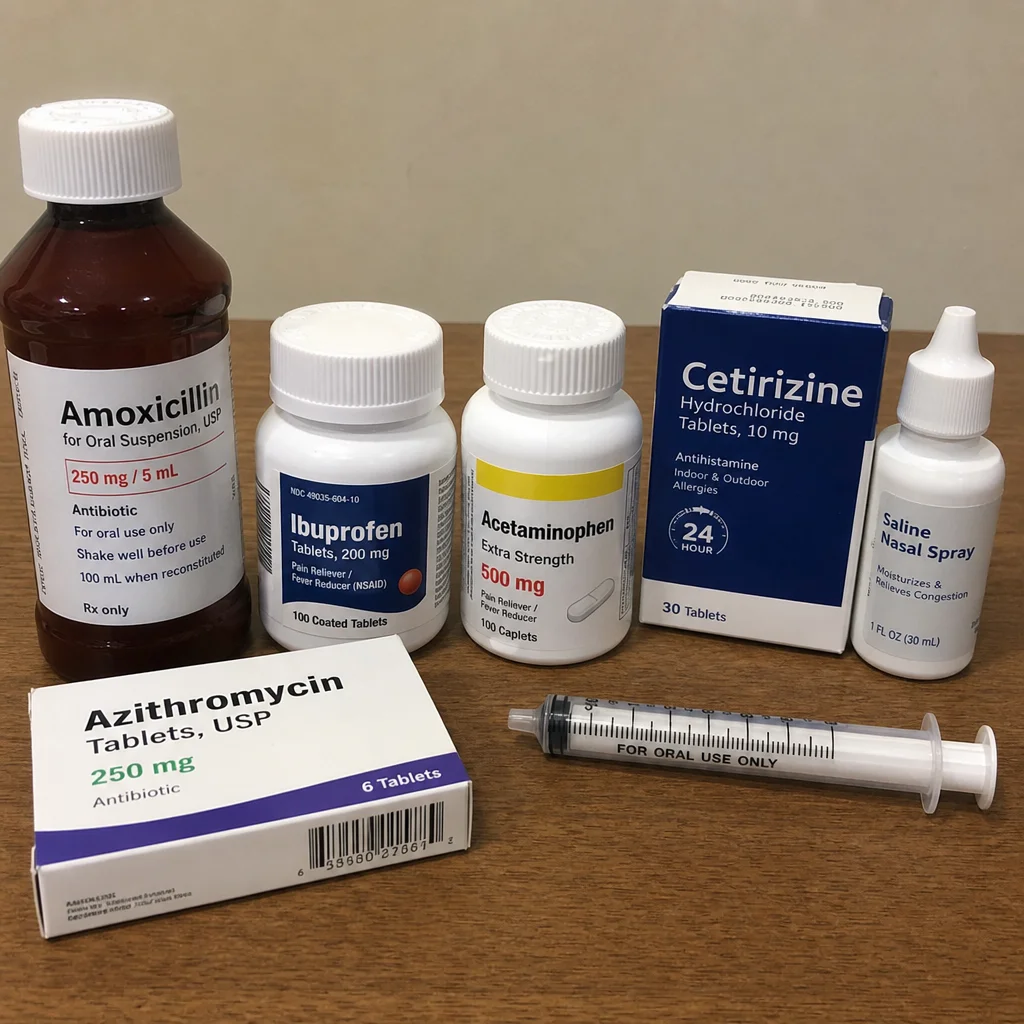
Over-the-Counter Analgesics: Non-steroidal anti-inflammatory drugs (NSAIDs) like ibuprofen or naproxen are excellent because they tackle both the pain and the inflammation causing the pressure. Acetaminophen is also effective for pain and fever reduction, though it lacks anti-inflammatory properties.
Warm Compresses: Applying a warm, moist washcloth or a moderately heated heating pad to the affected ear can relax the surrounding muscles, increase blood flow, and provide soothing relief.
Sleeping Position: Elevating the head using an extra pillow can encourage gravity to help drain the Eustachian tubes and reduce the localized blood pressure in the ear, making sleeping much easier.
Safe Pain Relief for Children with Earaches
Treating children requires a gentler, more precise approach. Finding safe pain relief for children with earaches is paramount to avoiding accidental overdoses or complications.
Weight-Based Dosing: Always use children’s formulas of ibuprofen (for children over 6 months) or acetaminophen. Ensure you are dosing based on the child's weight, not just their age, and use the syringe provided with the medication for accuracy.
The Aspirin Warning: Never give aspirin to children or teenagers. Aspirin use in children during viral infections has been strongly linked to Reye’s syndrome, a rare but potentially life-threatening condition that causes swelling in the liver and brain.
Distraction and Comfort: Sometimes, simply holding the child upright (which reduces middle ear pressure) and rocking them can provide significant comfort.
Anesthetic Ear Drops: If the eardrum is not ruptured, doctors sometimes prescribe anesthetic ear drops (like benzocaine drops) to numb the eardrum temporarily. However, these are less commonly used today due to limited long-term efficacy.
Medical Interventions: The Great Antibiotic Debate
For decades, the standard protocol for any ear infection was an immediate prescription for antibiotics. Today, the medical community's approach has evolved significantly, focusing heavily on antibiotic stewardship to prevent drug resistance.
The "Watch and Wait" Approach
Many ear infections are viral and will resolve on their own. Therefore, a common question patients ask is: how long do ear infections last without antibiotics? For mild cases, the worst of the pain typically peaks within the first 24 to 48 hours. Without antibiotics, a standard, uncomplicated middle ear infection will generally begin to improve within 2 to 3 days, with the infection fully clearing in 1 to 2 weeks.
Because of this, major pediatric and medical organizations now recommend a "watchful waiting" approach for 48 to 72 hours for:
Children aged 6 to 23 months with mild inner ear pain in only one ear.
Children 2 years and older with mild symptoms in one or both ears.
Adults with mild, manageable symptoms.
During this waiting period, aggressive pain management is the primary focus. If symptoms worsen or do not improve after 72 hours, antibiotics are then introduced.
Antibiotics for Ear Infection in Adults and Children
If watchful waiting fails, or if the infection is severe from the outset (high fever, severe pain, bilateral infection in young toddlers), antibiotics are necessary.
The first-line defense is almost universally Amoxicillin, a penicillin-based antibiotic. It is highly effective against the most common bacterial strains that cause otitis media.
For Children: It is usually given in a high-dose liquid form for 5 to 10 days, depending on the child's age and the severity of the infection.
Antibiotics for ear infection in adults: Adults may be prescribed amoxicillin or, if the infection is stubborn, Amoxicillin-clavulanate (Augmentin). Adults typically take pill forms for 5 to 7 days.
Crucial Advice on Antibiotics: If you are prescribed antibiotics, you must finish the entire course, even if you feel 100% better after two days. Stopping early leaves the strongest, most resistant bacteria alive in the ear, leading to a much harder-to-treat recurrent infection.
Eustachian Tube Management
Because almost all middle ear issues originate from a blocked Eustachian tube, directly addressing this blockage is a highly effective supplementary otitis-media-infection-treatment.
Proper Eustachian tube dysfunction management can speed up the drainage of fluid:
Nasal Decongestants: Over-the-counter nasal sprays (like oxymetazoline) can rapidly reduce swelling in the nasal passages and the opening of the Eustachian tube. However, they should not be used for more than 3 consecutive days to avoid "rebound congestion."
Oral Decongestants: Medications containing pseudoephedrine can help dry up secretions, though they may cause jitteriness or elevated heart rate in some adults.
The Valsalva Maneuver: This simple technique involves pinching your nose, closing your mouth, and gently blowing out (like you are blowing up a balloon). This forces air up the Eustachian tube, often resulting in a satisfying "pop" that equalizes pressure. Note: Do not do this forcefully, as it can damage the eardrum.
Hydration: Drinking plenty of water thins out mucus, making it easier for the Eustachian tubes to drain naturally.
Natural and Home Remedies for Ear Fluid
While serious bacterial infections require medical intervention, many people prefer to complement their care with holistic approaches, especially when dealing with the lingering fluid of Otitis Media with Effusion.
If you are looking for natural remedies for fluid behind ear, consider the following safe options:
Steam Inhalation: Breathing in steam from a bowl of hot water or taking a hot, steamy shower can work wonders for opening up congested respiratory and auditory passages. Adding a drop or two of eucalyptus or peppermint essential oil to the water can enhance the decongestant effect.
Garlic Oil Drops: Garlic has natural antimicrobial and anti-inflammatory properties. Warm (not hot) garlic oil dropped into the ear canal can soothe pain. Warning: Never put liquids or oils into the ear if you suspect the eardrum is ruptured or if the patient has ear tubes.
Chewing Gum or Yawning: The physical act of chewing and swallowing activates the muscles that open the Eustachian tube. Chewing sugar-free gum is an excellent way for adults and older children to encourage drainage. For infants, feeding or offering a pacifier achieves the same mechanical benefit.
Dietary Adjustments: Some holistic practitioners suggest reducing dairy intake during an active respiratory infection, as it can thicken mucus in some individuals, though scientific consensus on this varies.
Surgical Interventions: Ear Tubes (Tympanostomy)
For some unfortunate patients—usually young children—ear infections become a relentless cycle. When a child has three distinct ear infections in six months, or four in a single year, or if fluid remains trapped behind the eardrum for months causing hearing loss, a doctor will likely refer the patient to an Ear, Nose, and Throat (ENT) specialist.
The most common surgical otitis-media-infection-treatment is the insertion of tympanostomy tubes.
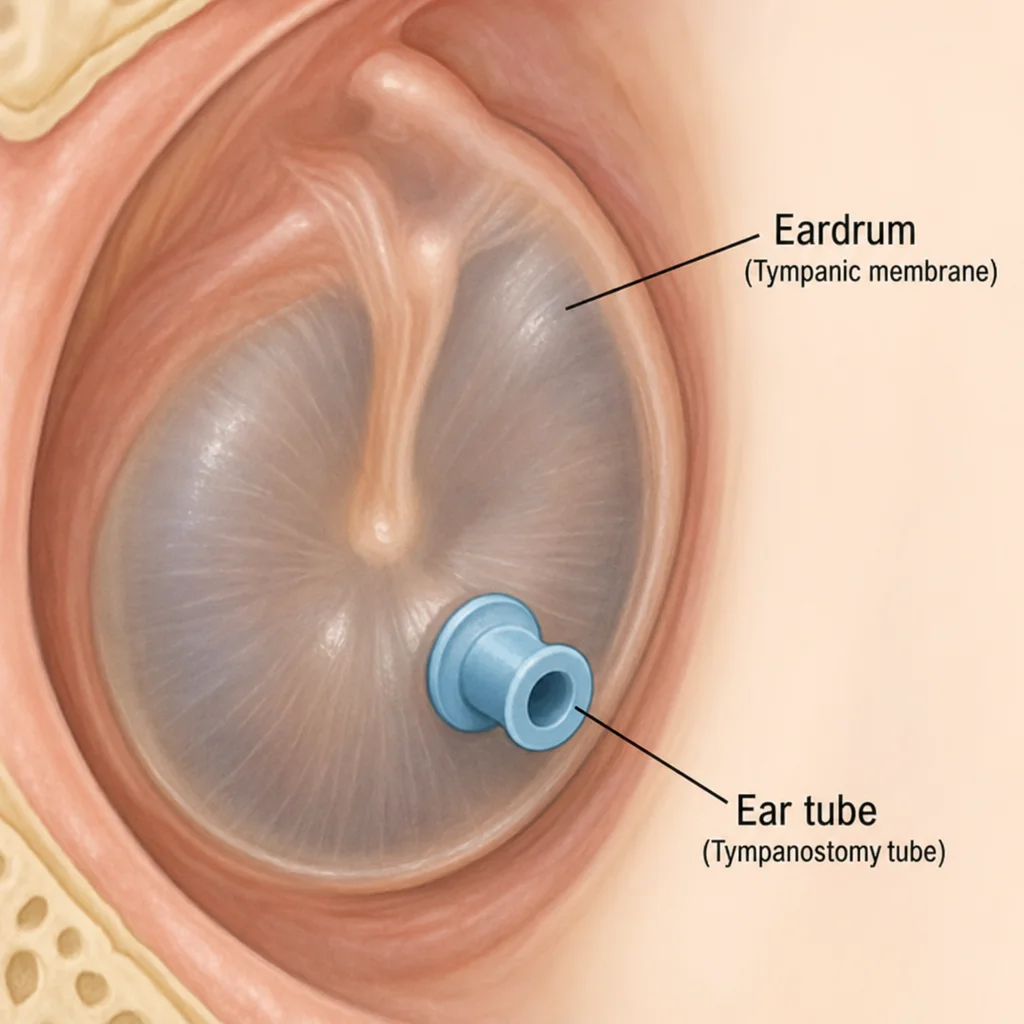
How the Surgery Works
The procedure is known as a myringotomy. Under light general anesthesia (for children) or local anesthesia (for adults), the surgeon makes a microscopic slit in the eardrum. They suction out the thick, trapped fluid (often called "glue ear") and insert a tiny, hollow cylinder (the ear tube) into the hole. This tube takes over the job of the failing Eustachian tube, allowing air to flow into the middle ear and fluid to drain out easily.
Ear Tube Surgery Pros and Cons
If you are considering this step, it is vital to weigh the ear tube surgery pros and cons:
The Pros:
Immediate Relief: The tubes instantly restore normal air pressure, immediately eliminating the pain and fullness.
Hearing Restoration: By clearing the fluid, hearing returns to normal instantly, which is crucial for a child’s speech and language development.
Drastic Reduction in Infections: While a child might still get an infection, the fluid will drain out the tube instead of building up and causing pain.
Easier Treatment: If an infection does occur with tubes in place, it can usually be treated with antibiotic ear drops directly into the ear, bypassing the need for systemic oral antibiotics.
The Cons:
Anesthesia Risks: While the procedure only takes about 10-15 minutes, it does require general anesthesia for children, which always carries minor risks.
Water Precautions: Depending on the type of tube, the doctor may recommend wearing earplugs while swimming in untreated water (like lakes or rivers) to prevent bacteria from entering the middle ear through the tube.
Premature Falling Out or Retention: Tubes are designed to fall out naturally as the eardrum heals (usually within 6 to 18 months). Sometimes they fall out too early (requiring a second surgery) or stay in too long (requiring surgical removal).
Scarring: Repeated tube surgeries can lead to tympanosclerosis, a minor scarring of the eardrum that usually does not affect hearing but is visible to a doctor.
Understanding the Risks: Complications of Untreated Infections
It is easy to dismiss an earache as a minor annoyance, but ignoring a severe infection can lead to profound health issues. The complications of untreated middle ear infections occur because the middle ear is surrounded by critical anatomical structures, including the brain, the mastoid bone, and facial nerves.
Hearing Loss from Middle Ear Fluid
The most common complication is hearing loss. Sound must vibrate the eardrum and the middle ear bones to be heard. When the middle ear is filled with thick, infected fluid, these vibrations are severely dampened.
Mild, temporary hearing loss from middle ear fluid is expected during an infection. However, if the fluid remains for months (Chronic OME), the prolonged hearing loss can have devastating effects on a developing child. It can lead to speech delays, poor school performance, and social isolation. Once the fluid is cleared, hearing usually returns to 100%, but the developmental time lost can be hard to recover.
Eardrum Rupture (Tympanic Membrane Perforation)
Sometimes, the pressure from the infected fluid becomes so immense that the eardrum simply bursts. While this sounds terrifying, patients actually report a sudden, massive relief from pain when a rupture occurs, followed by pus and blood draining from the ear canal.
Proper home care for ruptured eardrum is essential to ensure it heals correctly:
Keep the Ear Dry: Do not swim, and place a cotton ball coated in petroleum jelly in the outer ear while showering to keep water out.
Avoid Over-the-Counter Drops: Never put standard ear drops, oils, or hydrogen peroxide into a ruptured ear unless explicitly prescribed by a doctor, as these can enter the middle ear and cause severe damage or pain.
Watch for Infection: The doctor will likely prescribe antibiotic ear drops specifically formulated to be safe for a perforated eardrum (like Ofloxacin). Most ruptured eardrums heal on their own within two to four weeks.
Rare but Severe Complications
If an aggressive bacterial infection escapes the middle ear, it can cause:
Mastoiditis: An infection of the mastoid bone located just behind the ear. This causes redness, swelling behind the ear, and bone deterioration. It requires urgent intravenous antibiotics and sometimes surgery.
Facial Nerve Paralysis: The facial nerve runs closely adjacent to the middle ear. Severe inflammation can compress this nerve, leading to a drooping face on the affected side.
Meningitis: In incredibly rare cases, the infection can spread to the membranes surrounding the brain and spinal cord, which is a life-threatening medical emergency.
Staying Ahead: Prevention Strategies
The best otitis-media-infection-treatment is preventing the infection from occurring in the first place. While you cannot protect yourself or your children from every germ, implementing preventive measures for recurrent otitis media can dramatically reduce the frequency of infections.
1. Practice Vigorous Hygiene: Most ear infections start as a cold. Teaching children to wash their hands frequently and thoroughly, and keeping them away from visibly sick playmates, reduces their exposure to upper respiratory viruses.
2. Breastfeeding and Bottle Positioning: For infants, breast milk contains powerful, customized antibodies that help protect against ear infections. If you bottle-feed, always hold the baby in a semi-upright position. Propping a bottle while a baby is lying flat allows milk to easily pool in the back of the throat and flow into the Eustachian tubes, inviting bacterial growth.
3. Eliminate Exposure to Secondhand Smoke: Numerous studies have definitively linked secondhand smoke to a higher incidence of middle ear infections in children. Smoke paralyzes the tiny hair-like structures (cilia) inside the Eustachian tube that normally sweep mucus and debris away, causing fluids to back up.
4. Keep Vaccinations Up to Date: Certain vaccines play a massive role in preventing ear infections. The pneumococcal conjugate vaccine (PCV13 or PCV15) protects against Streptococcus pneumoniae, a leading cause of bacterial ear infections. Additionally, receiving an annual flu shot prevents the influenza virus, which frequently precedes a middle ear infection.
5. Manage Allergies Effectively: If you or your child suffer from environmental allergies (like pollen, dust mites, or pet dander), the constant inflammation and mucus production can keep the Eustachian tubes perpetually blocked. Working with an allergist to manage these symptoms via antihistamines, nasal corticosteroids, or immunotherapy can prevent the fluid buildup that leads to infections.
6. Pacifier Weaning: Research suggests a correlation between the continuous use of pacifiers in older infants/toddlers and an increased risk of ear infections. The constant sucking motion can alter pressure in the middle ear. Weaning a child off a pacifier after 6 to 12 months of age can serve as a helpful preventive step.
Making the Call: When to Seek Professional Help
While home care and watchful waiting are often appropriate, ear infections can escalate quickly. Knowing exactly when to see a doctor for earache is vital for preventing complications.
You should seek medical attention immediately if:
The patient is under 6 months old and shows any sign of ear pain or fever.
The pain is described as severe, intolerable, or worsening rapidly.
You notice blood, pus, or a foul-smelling fluid draining from the ear.
A fever of 102.2°F (39°C) or higher accompanies the earache.
The patient experiences sudden hearing loss, extreme dizziness, or a sensation that the room is spinning (vertigo).
There is visible swelling, redness, or tenderness on the skin behind the ear (a potential sign of mastoiditis).
Symptoms do not begin to improve after 48 to 72 hours of home care.
The patient appears exceptionally lethargic, stiff-necked, or unresponsive.
Your primary care physician or a pediatric specialist can properly examine the eardrum, accurately diagnose the specific type of otitis media, and formulate an aggressive, effective treatment plan tailored to the situation.
Conclusion
Navigating the pain and stress of a middle ear infection can be incredibly taxing, but you are not without options. From the sudden, sharp pains of Acute Otitis Media to the dull, lingering muffled hearing of Otitis Media with Effusion, understanding the mechanics of the ear is your first line of defense.
By familiarizing yourself with the symptoms—especially the subtle behavioral changes in toddlers—you can act swiftly. Whether your specific otitis-media-infection-treatment ends up involving a warm compress and ibuprofen, a strict course of antibiotics, or a conversation about ear tubes with an ENT specialist, knowledge is power.
Remember, the goal is always twofold: provide rapid pain relief and preserve long-term hearing health. By utilizing preventive measures, properly managing respiratory illnesses, and knowing exactly when to consult a medical professional, you can protect yourself and your loved ones from the complications of untreated middle ear infections. With the right care and patience, the pain will fade, the fluid will drain, and clear, painless hearing will return.