4 Types of Hearing Loss Explained: A Comprehensive Guide
Understanding the Four Types of Hearing Loss
Hearing connects us to the world around us. It allows us to participate in lively conversations, enjoy the complex melodies of a symphony, and stay alert to environmental sounds like a ringing phone or an approaching car. However, when hearing begins to fade, it can feel incredibly isolating.
Because hearing is an intricate physiological process, its deterioration is equally complex. There is no single "deafness" that applies to everyone. Instead, audiologists and medical professionals categorize auditory deficits into specific categories to tailor treatments effectively. Understanding the 4 types of hearing loss is the foundational step toward finding the right medical intervention, managing daily communication, and reclaiming your quality of life.
In this comprehensive guide, we will explore the anatomy of the ear, dive deep into the specific hearing impairment types, outline the actionable treatments available today, and help you decode the often-confusing medical jargon surrounding auditory health.
How We Hear: A Brief Primer on Ear Anatomy
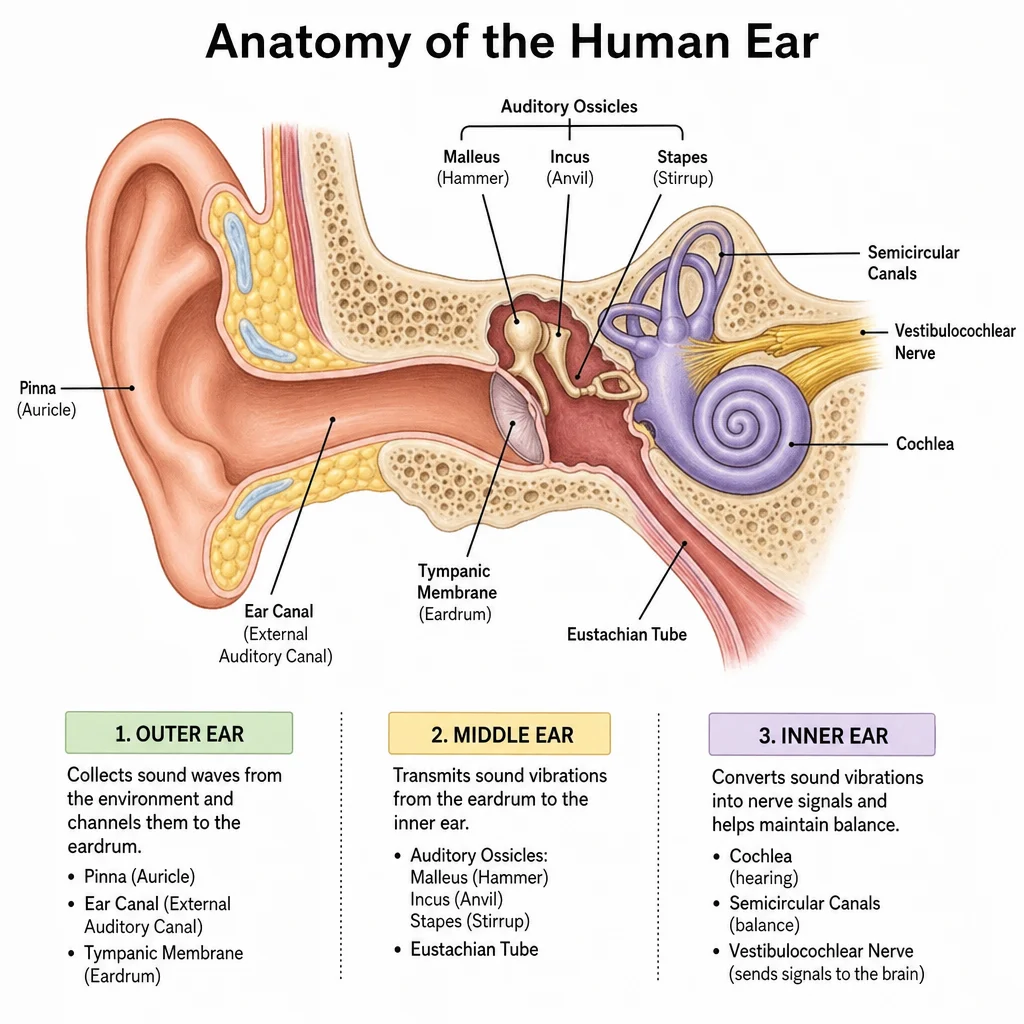
To truly grasp the different types of deafness and hearing conditions, it is crucial to first understand the journey of sound. Our ears are marvels of biological engineering, divided into three main sections:
The Outer Ear: Consists of the pinna (the visible part of the ear) and the ear canal. Its primary job is to catch sound waves from the environment and funnel them toward the eardrum.
The Middle Ear: Contains the tympanic membrane (eardrum) and three tiny bones called ossicles (the malleus, incus, and stapes). When sound waves hit the eardrum, it vibrates. These vibrations are amplified by the ossicles and pushed into the inner ear.
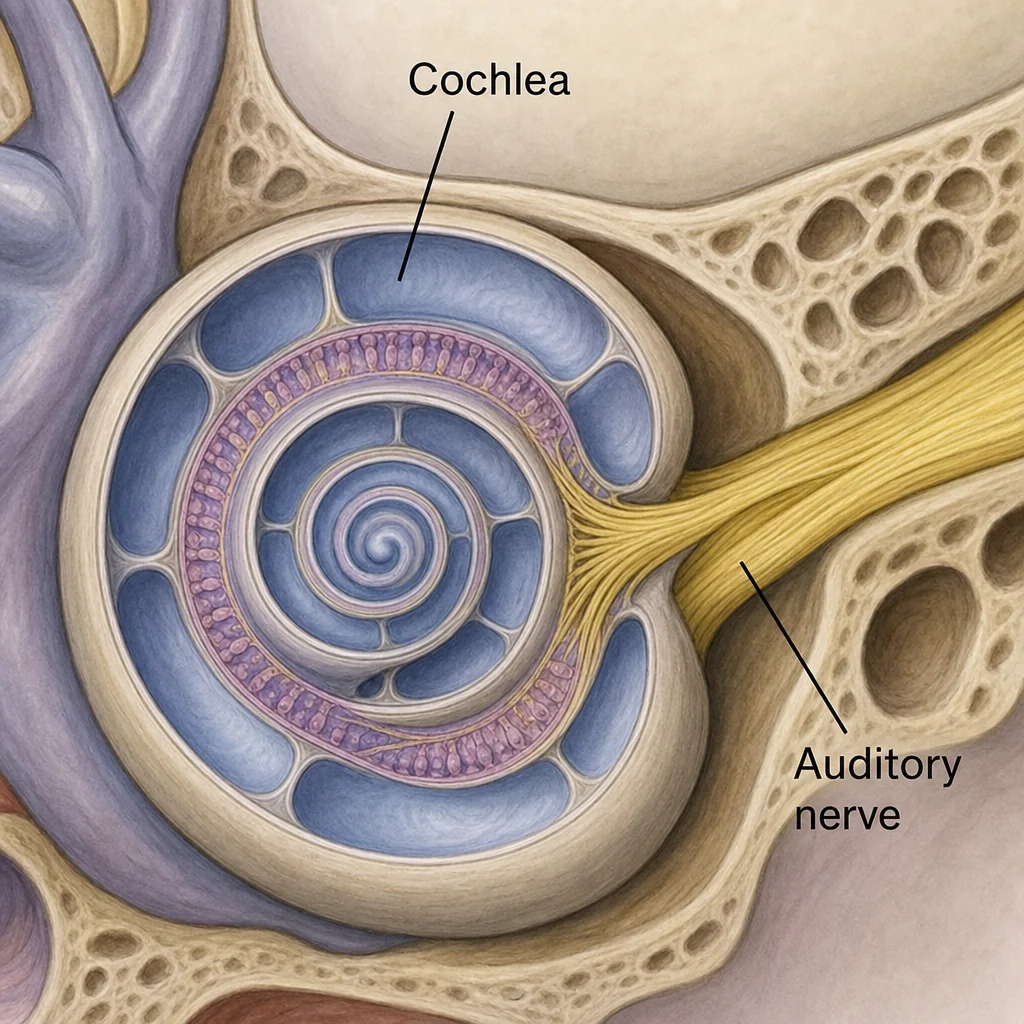
The Inner Ear: Home to the cochlea, a snail-shaped, fluid-filled structure lined with thousands of microscopic hair cells (stereocilia). The vibrations from the middle ear create waves in the cochlear fluid. These waves bend the hair cells, converting mechanical energy into electrical impulses that travel up the auditory nerve to the brain. The brain then translates these impulses into the sounds we recognize.
When a breakdown occurs at any point in this complex pathway, hearing loss is the result.
What Are the Degrees of Hearing Impairment?
Before exploring the biological causes of hearing loss, we must answer a common question: what are the degrees of hearing impairment?
Hearing loss is not a binary state of "hearing" or "deaf." Audiologists measure hearing acuity in decibels (dB), which represent the loudness of a sound. The degree of loss is determined by the quietest sound you can hear.
Normal Hearing (0 to 20 dB): You can hear quiet sounds like breathing or rustling leaves without effort.
Mild Hearing Loss (21 to 40 dB): Soft speech or distant conversations become difficult to understand, especially in environments with background noise.
Moderate Hearing Loss (41 to 70 dB): Normal conversational volume is hard to follow. You likely need a hearing aid to communicate effectively.
Severe Hearing Loss (71 to 90 dB): You may only hear loud noises, such as a vacuum cleaner or a dog barking close by. Conversations are impossible without amplification.
Profound Hearing Loss (91+ dB): You rely heavily on visual cues, sign language, lip-reading, or advanced surgical interventions. Even very loud sounds, like a lawnmower or airplane engine, are muffled or imperceptible.
Now that we have established the severity scales, let's delve into the 4 types of hearing loss: Sensorineural, Conductive, Mixed, and Auditory Neuropathy Spectrum Disorder.
Type 1: Sensorineural Hearing Loss (SNHL)
Sensorineural hearing loss (SNHL) is by far the most common of the 4 types of hearing loss, accounting for roughly 90% of all reported cases in adults. It occurs when there is damage to the inner ear (the cochlea) or to the neural pathways connecting the inner ear to the brain.
Because this type of loss stems from nerve or cellular damage, it is almost always permanent.
The Impact of Noise-Induced Hearing Damage on Inner Ear Hair Cells
One of the leading culprits of SNHL is noise exposure. The microscopic hair cells in the cochlea are incredibly fragile. To understand the impact of noise-induced hearing damage on inner ear hair cells, imagine a field of fresh green grass. If you walk across the grass once, it bends but springs back up. If a massive crowd stomps over the grass every day, the blades eventually break and die.
Similarly, single exposures to extremely loud sounds (like a gunshot) or prolonged exposure to moderately loud sounds (like heavy machinery or blasting music through headphones) permanently bend and destroy these hair cells. Because human beings cannot regenerate inner ear hair cells, once they die, the hearing loss is irreversible.
Sensorineural Hearing Loss Causes and Treatments
Aside from noise exposure, several other factors contribute to SNHL:
Presbycusis (Age-Related Hearing Loss): Natural wear and tear on the inner ear as we age.
Genetics: Hereditary traits that predispose individuals to early auditory decline.
Ototoxic Medications: Certain drugs—including specific antibiotics (like gentamicin), chemotherapy drugs, and even high doses of aspirin—can be toxic to the inner ear.
Viral and Bacterial Infections: Illnesses such as mumps, measles, meningitis, and cytomegalovirus (CMV).
Head Trauma: A severe blow to the head can fracture the temporal bone or damage the auditory nerve.
When it comes to sensorineural hearing loss causes and treatments, the primary goal is management and amplification rather than "curing" the disease.
Treatment Options Include:
Hearing Aids: Modern digital hearing aids are highly sophisticated. They do not just amplify all sound; they can be programmed to boost only the specific frequencies a patient struggles to hear while actively suppressing background noise.
Assistive Listening Devices (ALDs): FM systems, amplified telephones, and looping systems help bridge the gap in specific difficult listening environments.
Cochlear Implants: For individuals with severe-to-profound SNHL where hearing aids no longer provide a benefit.
Common Signs of High-Frequency Hearing Loss
SNHL often begins in the high-frequency range. This means you might pass a basic volume test but fail to hear specific pitches. The common signs of high-frequency hearing loss include:
Difficulty distinguishing consonant sounds, particularly s, f, th, sh, v, and p.
Feeling like everyone is mumbling.
Struggling to understand women's and children's voices (which naturally pitch higher than adult male voices).
Inability to hear birds chirping or the beeping of a microwave.
Exhaustion after social interactions (known as "listening fatigue") due to the immense brainpower required to fill in conversational blanks.
Sudden Sensorineural Hearing Loss Emergency Symptoms
While SNHL usually develops gradually over years, it can occasionally happen overnight. Sudden Sensorineural Hearing Loss (SSNHL), sometimes called sudden deafness, is a medical emergency.
If you experience sudden sensorineural hearing loss emergency symptoms, do not assume your ear is simply plugged with wax. These symptoms include:
A rapid, unexplained drop in hearing in one ear (often noticed upon waking up).
A feeling of intense fullness or pressure in the ear.
A loud, ringing, or roaring tinnitus.
Dizziness, vertigo, or a sudden loss of balance.
Immediate action is required. If treated within the first 48 to 72 hours with a high-dose course of oral or injected corticosteroids, the chances of recovering the lost hearing are significantly higher. Delaying treatment for weeks usually results in permanent loss.
Age-Related Hearing Loss Prevention Strategies
While we cannot stop the clock, we can protect the hearing we have. Implementing age-related hearing loss prevention strategies is vital for long-term auditory health:
Follow the 60/60 Rule: When listening to music with headphones, keep the volume at or below 60% of the maximum, and limit listening time to 60 minutes a day.
Wear Hearing Protection: Keep earplugs handy for concerts, sporting events, or when operating power tools. Custom-molded earplugs offer excellent protection without distorting sound fidelity.
Manage Cardiovascular Health: The inner ear relies on robust blood flow to survive. High blood pressure, diabetes, and smoking can restrict blood vessels, accelerating hair cell death. Regular exercise and a heart-healthy diet directly protect your ears.
Review Medications: Always ask your doctor or pharmacist if a newly prescribed medication is ototoxic, and inquire about alternatives if necessary.
Type 2: Conductive Hearing Loss
The second of the 4 types of hearing loss is Conductive Hearing Loss (CHL). Unlike SNHL, which involves nerve damage, conductive loss is a mechanical problem. It occurs when sound waves are physically blocked from passing through the outer ear, the middle ear, or both.
Imagine trying to look out of a window with the blinds pulled down. The world outside is still there (the inner ear works fine), but the light is obstructed from entering.
Difference Between Conductive and Sensorineural Hearing Loss
Understanding the difference between conductive and sensorineural hearing loss is essential for determining the correct treatment path.
Location: Conductive loss happens in the outer/middle ear. Sensorineural loss happens in the inner ear/auditory nerve.
Sound Quality: People with conductive loss often feel that all sounds are simply "turned down" or muffled. If the volume is made loud enough, they can hear clearly. People with sensorineural loss experience distortion. Even if you make a sound louder, it may still sound garbled or unintelligible.
Self-Perception: Interestingly, someone with conductive hearing loss often speaks very softly. Because the blockage prevents outside noise from getting in, their own voice resonates loudly in their head (the occlusion effect). Conversely, someone with SNHL may speak very loudly because they cannot monitor the volume of their own voice.
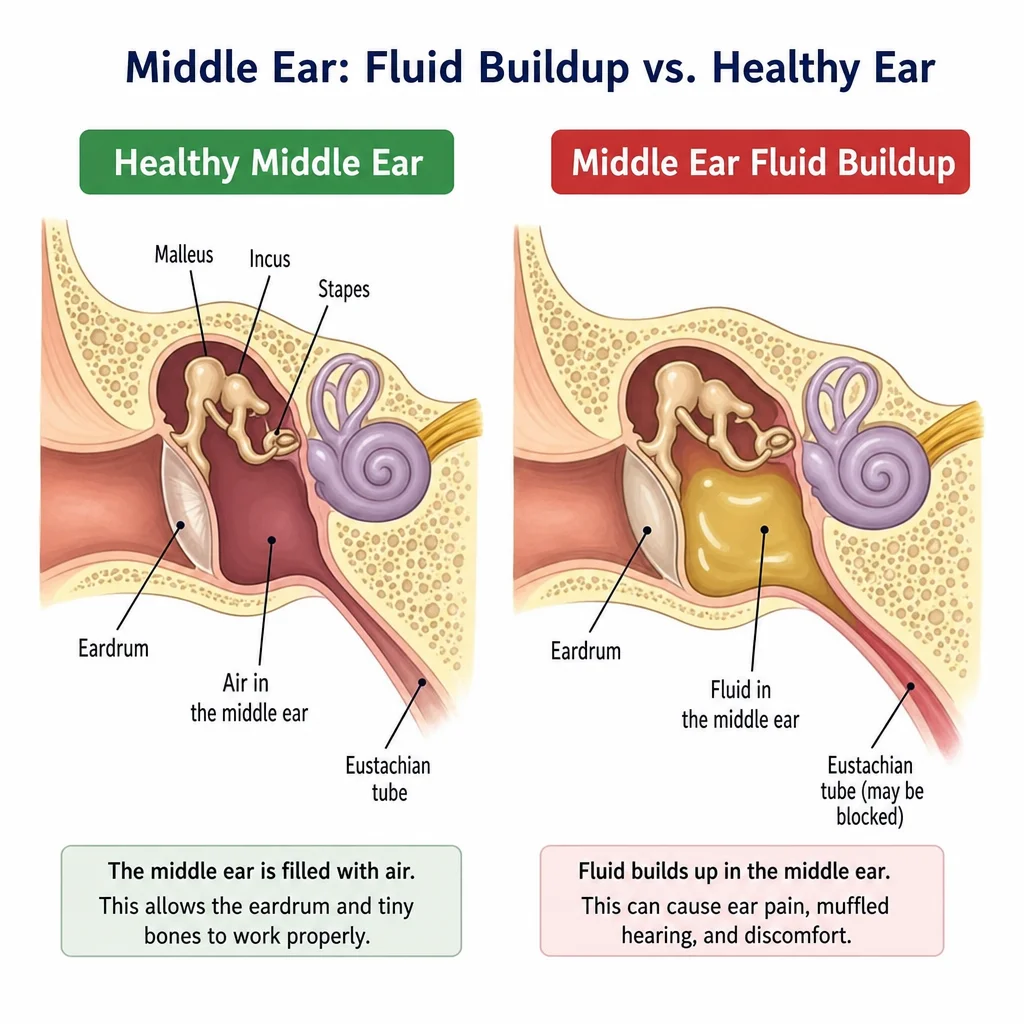
Middle Ear Infection and Temporary Hearing Impairment
One of the most frequent causes of conductive hearing loss, especially in children, is Otitis Media. This links directly to the concept of middle ear infection and temporary hearing impairment.
When an individual gets a cold or allergies, the Eustachian tube (which connects the middle ear to the back of the throat) can swell and become blocked. Fluid then becomes trapped behind the eardrum. Because sound waves struggle to travel through thick fluid compared to air, hearing is significantly muffled. Once the infection clears—often with the help of antibiotics or the insertion of tiny tympanostomy tubes to drain the fluid—hearing typically returns to normal.
Other Causes of Conductive Hearing Loss
Besides fluid, several other factors can cause a conductive blockage:
Cerumen Impaction: A severe buildup of earwax in the ear canal.
Foreign Objects: Common in toddlers who may stick beads or food into their ears.
Perforated Eardrum: A tear in the tympanic membrane caused by trauma, loud blasts, or severe infections.
Otosclerosis: An abnormal bone growth in the middle ear that fuses the stapes bone, preventing it from vibrating.
Microtia or Atresia: Congenital deformities where the outer ear is malformed or the ear canal is completely closed off.
Can Conductive Hearing Loss Be Reversed?
A common question patients ask is, "Can conductive hearing loss be reversed?" The answer, in the vast majority of cases, is yes.
Because conductive hearing loss is a mechanical obstruction, medical or surgical interventions are highly successful.
Earwax removal: A simple, painless procedure performed by a doctor using microsuction or irrigation restores hearing instantly.
Medication: Antibiotics or antifungal drops can resolve infections causing swelling and blockages.
Surgery: Procedures like a tympanoplasty can patch a hole in the eardrum, while a stapedectomy can replace a fused middle ear bone with a tiny prosthetic, instantly restoring the mechanical vibration pathway.
Bone-Anchored Hearing Systems for Outer Ear Problems
In cases where conductive hearing loss cannot be surgically corrected—such as severe chronic ear infections, allergic reactions to traditional hearing aids, or congenital atresia (missing ear canal)—specialized technology steps in.
Bone-anchored hearing systems for outer ear problems (often referred to as Baha devices) are life-changing. These devices bypass the outer and middle ear entirely. A tiny titanium implant is placed into the skull behind the ear. An external sound processor attaches to this implant. When the processor picks up sound, it translates it into physical vibrations that travel directly through the skull bone into the healthy, functioning cochlea.
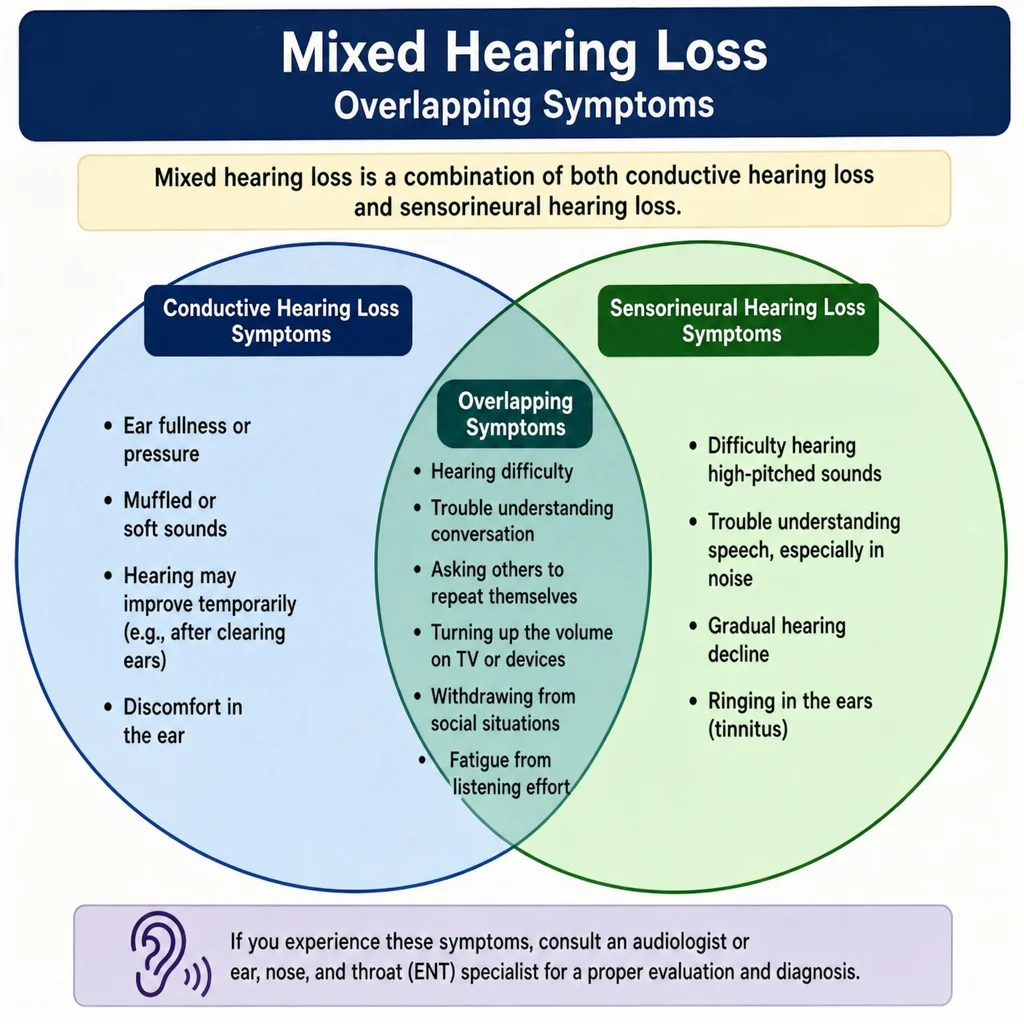
Type 3: Mixed Hearing Loss
Sometimes, auditory issues do not fit neatly into a single category. The third classification is Mixed Hearing Loss.
Mixed hearing loss is exactly what it sounds like: a combination of both conductive and sensorineural hearing damage occurring in the same ear. This means there is damage in the outer or middle ear and in the inner ear or auditory nerve.
Real-World Examples of Mixed Hearing Loss
To illustrate, consider an older gentleman who has worked in a loud factory for 30 years and has naturally developed age-related and noise-induced sensorineural hearing loss. One day, he develops a severe outer ear infection (Swimmer’s ear) that swells his ear canal shut. He now has a mixed hearing loss: the permanent inner ear damage combined with the temporary conductive blockage.
Another example is an individual who suffers a severe head trauma that simultaneously fractures the tiny bones of the middle ear (conductive) and damages the delicate hair cells in the cochlea (sensorineural).
Mixed Hearing Loss Management Options
Treating mixed hearing loss requires a multi-tiered approach. Audiologists and Ear, Nose, and Throat (ENT) specialists must collaborate to tackle the issue.
The standard protocol for mixed hearing loss management options is to address the conductive component first.
Medical/Surgical Intervention: The physician will clear out earwax, treat any infections with antibiotics, or perform surgery to repair a perforated eardrum or damaged ossicles.
Re-evaluation: Once the conductive barrier is removed or minimized, the patient undergoes another hearing test to determine the exact degree of the remaining, permanent sensorineural loss.
Amplification: Finally, the audiologist will fit the patient with appropriate hearing aids to treat the remaining sensorineural deficit.
In some cases, if the conductive component is permanent, bone-anchored hearing systems or specialized middle-ear implants can be utilized to treat both issues simultaneously by amplifying vibrations directly into the skull.
Type 4: Auditory Neuropathy Spectrum Disorder (ANSD)
The fourth and most complex of the 4 types of hearing loss is Auditory Neuropathy Spectrum Disorder (ANSD). While less common than SNHL or conductive loss, it is vital to understand because it behaves entirely differently.
Auditory Neuropathy Spectrum Disorder Explained
To get auditory neuropathy spectrum disorder explained simply, we must look at the brain's role in hearing. In ANSD, the outer, middle, and even the inner ear (specifically the outer hair cells of the cochlea) are perfectly healthy and function normally. The ear detects the sound without issue.
The problem arises in the transmission of that sound from the inner ear to the brain. The inner hair cells or the auditory nerve itself become out of sync. They fail to fire electrical impulses in a coordinated, organized manner (a condition known as dyssynchrony).
Imagine a beautiful, high-definition television receiving a corrupted, scrambled broadcast signal. The TV itself is fine, but the picture is a pixelated, static mess. This is what individuals with ANSD experience with sound.
People with ANSD can often "hear" sounds—meaning they know a noise occurred—but they cannot comprehend it. Speech may sound incredibly garbled, fading in and out of clarity. Because of this, traditional pure-tone hearing tests often fail to capture the severity of the disability. An individual might show perfectly normal hearing levels on an audiogram but have zero speech comprehension.
Diagnostic Tests for Auditory Processing Issues
Because traditional behavioral hearing tests are insufficient for detecting ANSD, audiologists must rely on objective, physiological measurements. The most critical diagnostic tests for auditory processing issues and neuropathy include:
Otoacoustic Emissions (OAEs): A tiny probe is placed in the ear canal to measure the acoustic response of the outer hair cells in the cochlea. In a patient with ANSD, OAEs are typically present and robust, proving the cochlea is healthy.
Auditory Brainstem Response (ABR): Electrodes are placed on the patient's head to measure the brainwaves as they react to clicking sounds played in the ear. In a patient with ANSD, the ABR will be severely abnormal or completely absent, proving the neurological signal is failing to reach the brain coherently.
When OAEs are normal but the ABR is absent, an official diagnosis of Auditory Neuropathy is made. Treatment for ANSD is highly individualized. Some patients benefit from mild-gain hearing aids with FM systems to boost the signal-to-noise ratio. However, many eventually transition to cochlear implants, which bypass the damaged inner hair cells and directly stimulate the auditory nerve with a clearer, more synchronized electrical signal.
Deciphering the Jargon: Diagnosing Hearing Loss
Now that we have covered the specific medical classifications, how do doctors figure out which type you have? The answer lies in the audiogram.
How to Read an Audiogram Results
After a comprehensive hearing test in a soundproof booth, your audiologist will hand you a graph. To the untrained eye, it looks like a scattering of X's and O's. However, learning how to read an audiogram results empowers you to understand your own auditory health.
An audiogram is a graph that charts your hearing sensitivity.
The Axes:
The Horizontal Axis (X-axis): Represents Frequency, or pitch, measured in Hertz (Hz). It reads left to right, going from low pitches (like a bass drum at 250 Hz) to high pitches (like a whistling bird at 8000 Hz). Think of it like the keys on a piano.
The Vertical Axis (Y-axis): Represents Intensity, or loudness, measured in decibels (dB). It reads top to bottom. The top of the graph (0 dB) represents very soft sounds. The bottom of the graph (100+ dB) represents very loud sounds.
The Symbols:
Red Circle (O): Represents the hearing threshold for the Right ear using air conduction (standard headphones).
Blue 'X' (X): Represents the hearing threshold for the Left ear using air conduction.
Brackets ([ or ]): Represent bone conduction testing. A vibrating headband is placed behind the ear, bypassing the outer/middle ear entirely to test only the cochlea.
Determining the Type of Hearing Loss:
Sensorineural: Both the X/O symbols and the bone conduction brackets show hearing loss at the same levels. This proves the issue is entirely in the inner ear.
Conductive: The bone conduction brackets show normal hearing (meaning the cochlea is healthy), but the X/O symbols show hearing loss. The gap between these two scores (called an air-bone gap) proves there is a mechanical blockage in the outer or middle ear.
Mixed: Both the bone conduction brackets and the X/O symbols show hearing loss, but the X/O symbols are much worse.
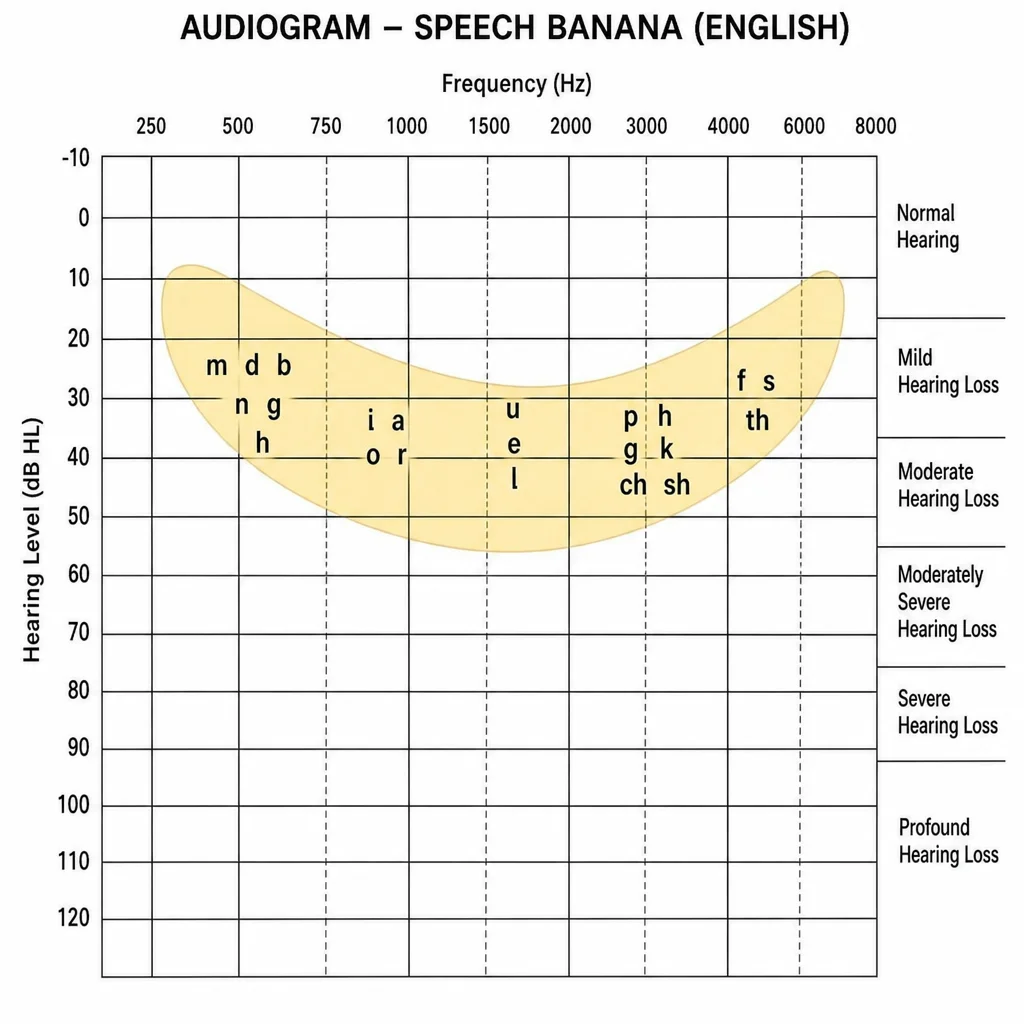
The Speech Banana: Many audiograms feature a shaded, banana-shaped region in the middle of the graph. This represents where the sounds of normal human speech occur in terms of frequency and decibel level. If your X's and O's drop below this banana shape, it indicates you are missing critical conversational cues.
Advanced Treatment Technologies
Treating auditory deficits relies heavily on the specific classification of the loss. As we advance further into the 21st century, technological solutions continue to break boundaries.
Cochlear Implants vs Hearing Aids for Profound Loss
For individuals suffering from severe to profound sensorineural hearing loss, traditional hearing aids eventually hit a wall of diminishing returns. This brings us to a major clinical crossroads: cochlear implants vs hearing aids for profound loss.
Hearing Aids: These are essentially miniature, highly advanced amplifiers. They capture sound, make it louder, shape it to your specific prescription, and send it down your ear canal. However, if the hair cells in your inner ear are completely dead, no amount of volume will make the sound clear. It is like turning up the volume on a blown-out speaker; it just gets louder and more distorted.
Cochlear Implants: These are radically different. A cochlear implant does not amplify sound. It is a surgically implanted neuroprosthetic device. A surgeon threads a microscopic array of electrodes directly into the cochlea. An external processor worn behind the ear captures sound and turns it into digital signals. These signals bypass the dead hair cells entirely and directly stimulate the auditory nerve with electrical impulses.
The Verdict: While hearing aids are non-invasive and the first line of defense, a cochlear implant is the gold standard for individuals with profound SNHL who score poorly on speech recognition tests even with the best hearing aids. The rehabilitation process for a cochlear implant is intensive—the brain must literally learn a new way to "hear" electrical signals—but the outcome can restore a remarkable degree of speech comprehension.
Living With Hearing Loss: Practical Communication Strategies
Understanding the medical nuances of your diagnosis is only half the battle. Regardless of whether you have sensorineural, conductive, mixed, or auditory neuropathy, integrating practical communication strategies into your daily routine is vital for maintaining your mental health and relationships.
Hearing loss is often called the "invisible disability" because, unlike a cast on a broken arm, people cannot see it. Therefore, self-advocacy is key.
Face-to-Face Communication: Always ensure you can see the face of the person speaking to you. Even if you do not actively "lip-read," the brain automatically gathers immense amounts of phonetic information from lip movements and facial expressions to fill in auditory gaps.
Optimize Your Environment: In restaurants or public spaces, try to sit with your back to the wall. This minimizes the amount of background noise coming from behind you and allows your directional hearing aids to focus on the conversation in front of you. Request well-lit tables to aid visual cues.
Educate Family and Friends: Teach your loved ones that shouting does not help. Shouting distorts the face and makes the voice pitch higher, which is often harder for those with high-frequency SNHL to process. Instead, ask them to speak slowly, clearly, and to make sure they have your attention before starting a sentence.
Utilize Captioning: Embrace closed captioning on televisions, real-time transcription apps on smartphones, and captioned telephones to relieve the cognitive load of constant, strained listening.
Conclusion
The journey through the human auditory system reveals an incredibly delicate and complex biological process. When that system fails, it does not do so in just one way. By classifying deficits into the 4 types of hearing loss—Sensorineural, Conductive, Mixed, and Auditory Neuropathy Spectrum Disorder—audiologists can precisely target the root cause of the problem.
Whether it involves adopting age-related prevention strategies, treating an acute middle ear infection, relying on the acoustic brilliance of modern hearing aids, or undergoing life-altering surgery for a cochlear or bone-anchored implant, the pathways to better hearing are more robust today than at any point in history.
If you suspect that you or a loved one are missing out on the rich tapestry of sound that surrounds us, do not wait. Hearing loss is not just an ear issue; untreated, it links to cognitive decline, social isolation, and depression. Book an appointment with an audiologist, get a comprehensive evaluation, and take the first step toward reconnecting with the world. Your hearing is a precious resource—protect it, understand it, and nurture it.